
Scapulohumeral Rhythm
By: Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMS
The shoulder is one of the most vulnerable joints in the body due to its vast range of motion and complexity. It is a complex ball and socket joint, uniquely comprised of various connective tissue, supporting structures, including muscles. It is an important joint because functionally, it is involved in most daily and sport activities, such as reaching, lifting, carrying and throwing a ball. Knowledge of the biomechanics of the shoulder can help you with training and aiding in the rehabilitation of the shoulder and related injuries.
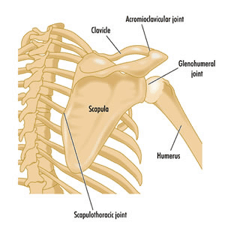
The shoulder complex involves coordinated movements between the humerus bone and the scapula. The scapula, clavicle, and humerus serve as attachments for most of the muscles in the shoulder. The shoulder is comprised of four primary joints (Figure 1):
- Glenohumeral joint (GH)
- Acromioclavicular joint (AC)
- Sternoclavicular joint (SC)
- Scapulothoracic joint
Scapulohumeral Rhythm (SHR) is defined as the movement relationship between the humerus and the scapula during both shoulder flexion and shoulder abduction. Arthrokinematics is the movement that takes place between articular surfaces in a joint.
For example, during abduction of the arm at the shoulder (side arm raise) the following happens (Figure 2):
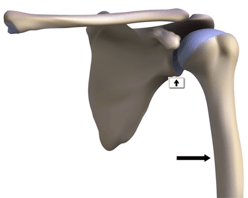
- The glenohumeral joint (concave) is stable (depicted by the vertical arrow), while the humerus (convex) abducts (depicted by the horizontal arrow).
- There is a sliding down or glide of the convex humerus on the concave glenohumeral joint.
- The scapula rotates upward (bottom of the scapula moves laterally and upward).
During shoulder abduction, there is 120 degrees of movement that occurs at the glenohumeral joint, while 60 degrees occurs at the scapulothoracic joint, creating a 2 to 1 ratio (2:1). This movement is known as the scapulohumeral rhythm (SHR) of shoulder abduction.
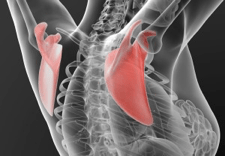
The same SHR occurs both during shoulder flexion and shoulder abduction (Figure 3).
The muscle actions that occur when you abduct the arm at the shoulder include:
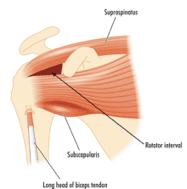
- Biomechanically, the supraspinatus muscle (Figure 4) raises the arm during the first 15 degrees of shoulder abduction.
- Then, from 15-90 degrees of shoulder abduction, the medial deltoid assists to raise the arm biomechanically.
- There are several muscles within the shoulder that play important roles, specifically at the rotator cuff. The rotator cuff is comprised of four primary muscles known as the S.I.T.S muscles. These muscles include the supraspinatus, infraspinatus, teres minor and subscapularis which pull the bone in different directions due to different attachment points and angle of pull.
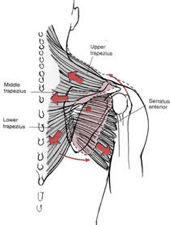
- A force couple can be defined as a pair of muscle forces that act together on a joint to produce rotation. These forces may exert pulls in opposite directions. Force couples may be synergistic pairs or agonist/antagonist pairs of muscles. In Figure 5, a force couple occurs between the low trapezius and serratus anterior. During shoulder abduction, the lower trapezius and serratus anterior work together to anterior upwardly rotate the scapula on the thorax.
Abnormal scapulohumeral rhythm is a dysfunction that occurs within the scapulothoracic junction.
There are many causes for this including:
- A rotator cuff tear where the individual does not have the musculotendinous connection and strength to abduct the arm.
- Limitations due to joint and capsule hypomobility (restriction) known as adhesive capsulitis (frozen shoulder).
- Pain and/or muscular weakness that prevent the ability to raise the arm to the side.
- Occurrence of excessive upper trapezius and scapular elevation which becomes a means of compensation, and provides the individual with an alternative ability to abduct the arm.
Why is this important?
- Connective tissue (muscles, tendons, ligaments, and fascia) are supposed to move. Joints, as well, have a certain amount of movement and should glide and translate with everyday movement.
- Muscle imbalances and tightness create dysfunction. If a muscle does not have adequate muscle length to concentrically and eccentrically contract, compensation will occur typically above and below a joint.
- If this tightness continues, it will result in trigger points. Trigger points are where a muscle shortens and, in essence, has increased sensitivity affecting the muscle’s ability to completely move as it was designed. If trigger points become bigger and more prominent, they can compress the nerve that innervates the respective muscle creating radicular (fuzzy feeling, numbness, or tingling) symptoms.
If the scapula is not able to properly upwardly rotate on the thorax, an individual will compensate using other muscles to perform the work. This compensation will lead to muscle imbalance, pain, and dysfunction affecting activities of daily living and sports movements.
For more information about working with clients with shoulder issues, see the Fitness Learning Systems Human Movement Matrix: Shoulder continuing education course by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMS of Pinnacle Training & Consulting Systems. www.pinnacle-tcs.com “Teaching The Science Behind The Movement.” Fitness Learning Systems is an IACET accredited continuing education provider.




No comment yet, add your voice below!